Having surgery is scary, even if it is a minimally-invasive procedure. Oftentimes, it’s not only the surgery itself people are concerned about, but the recovery period as well. While minimally-invasive gynecological surgery has the benefit of a faster and easier recovery than traditional open surgery, many women still have questions about the recovery process and what they should expect after surgery. Here are some of the most commonly asked questions regarding the recovery process, as well as some information on what to expect after having minimally-invasive gynecological surgery:
Q: How many incisions can I expect after minimally-invasive gynecological surgery?
A: One of the main benefits of using a minimally invasive approach is that the size of the incision will be greatly reduced when compared to incisions used for open surgery. However, while these incisions are much smaller, there may be approximately 3-5 tiny incisions. In most cases, these incisions are about 5mm across, which is roughly the size of a pencil eraser. Not only do smaller incisions heal faster, but they leave smaller and less noticeable scars.
Q: Do minimally-invasive procedures require a hospital stay?
A: In most cases, minimally-invasive surgical procedures are performed on an outpatient basis. This means that you will arrive at a hospital or surgery center for the procedure, spend about an hour or two in recovery, and then be discharged to recover in the comfort of your own home. Returning home after surgery lowers your risk of blood clots or contracting an infection from the hospital. However, there are some cases where your doctor may recommend staying a night or two in the hospital.
Q: When can I leave the hospital after surgery?
A: As mentioned above, most patients who have minimally-invasive surgery can leave the hospital after surgery. However, you will need to accomplish three things before being discharged. After surgery, you can leave the hospital once you can walk without assistance, are comfortable with pain medications, and can drink liquids without significant nausea.
Q: Can I drive after having minimally-invasive surgery?
A: No, you will need to have a driver take you home after surgery. Although minimally-invasive surgery is less stressful on your body than traditional open surgery, it is still important to let your body rest immediately after surgery. Additionally, it is not safe to drive after using the anesthetic and sedation used during minimally invasive-procedures.
Q: What can I expect in the days immediately following surgery?
A: In the days immediately following surgery, you can expect to experience some discomfort and possible swelling. To manage any postoperative discomfort, your doctor will prescribe pain medications, as well as medications to reduce inflammation. The good news is that minimally-invasive techniques minimize the trauma to the surrounding tissues and muscles, so any discomfort should resolve relatively quickly. Still, it is recommended to take it easy for the first few days after surgery.
Q: How long until I can return to my usual routine?
A: Most women are able to return to work within 1-3 weeks after their surgery. However, you will need to avoid lifting heavy objects or strenuous activities for at least six weeks after surgery to give your body a chance to heal completely. With the exception of heavy lifting or strenuous activities, most women return to a normal routine within two weeks following surgery.
If your gynecologist has recently recommended minimally invasive gynecological surgery, you are probably wondering just what that entails. Most people are aware of the fact that any type of minimally invasive surgery is less invasive, which means it causes less trauma, uses smaller incisions, and has shorter recovery times than traditional open surgery. However beyond this, there are probably many things about minimally invasive gynecological surgery that you don’t know. In fact, one common thing that many women don’t know about minimally invasive gynecological surgery is that there are three different types, including:
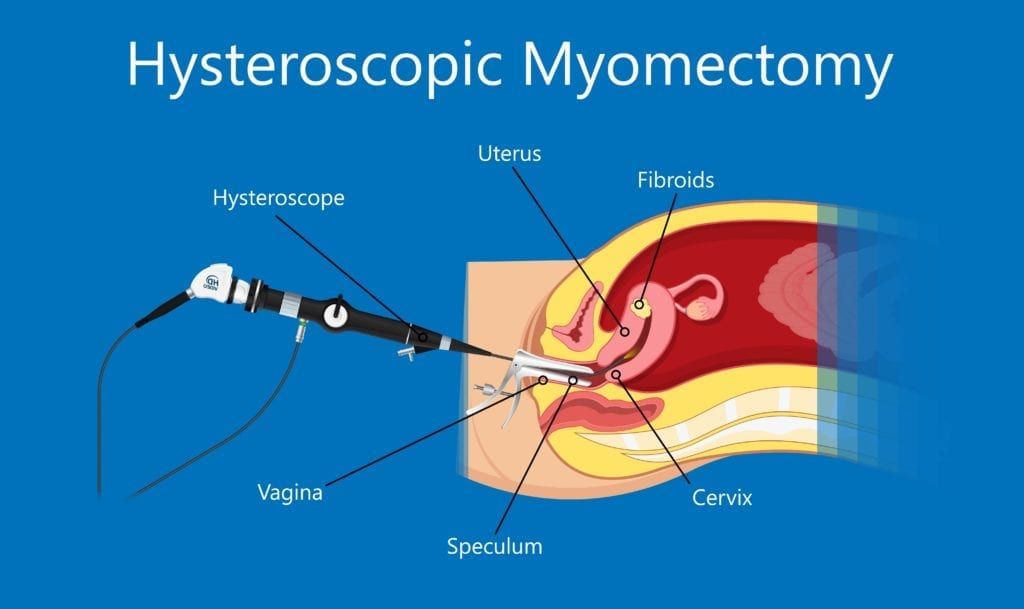
Hysteroscopic Procedures
These procedures use a hysteroscope, which is a long, telescopic instrument that is inserted through the vagina and cervix until it reaches the uterus. Once in the uterus, the hysteroscope can be used to obtain magnified views of the uterus. Surgical instruments can also be passed through the hysteroscope in order to execute treatment.
Hysteroscopies are generally performed to explore the inside of your cervix and uterus when you are experiencing heavy menstrual bleeding and/or severe cramps, have had one or more miscarriages, or to diagnose fibroids, polyps, or scarring on the uterus. They can also be performed as a way to obtain a biopsy when you have an abnormal Pap result, as a sterilization procedure for permanent birth control, or to fix a misplaced IUD.
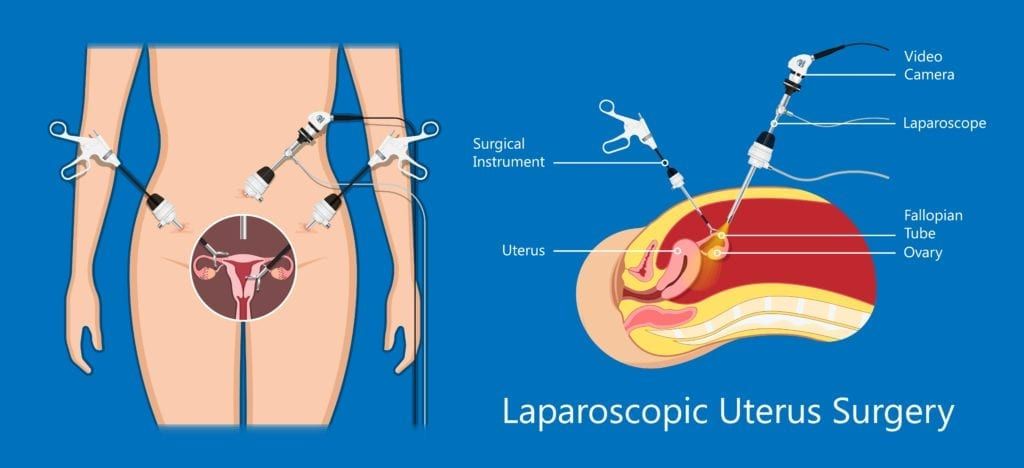
Laparoscopic Procedures
These procedures use a laparoscope, which is a long, telescopic instrument with a camera at the end, as well as 2 or 3 surgical instruments. The laparoscope is generally inserted through an incision in the belly button, while the surgical instruments are inserted through small incisions in the abdomen. The laparoscope provides a detailed video image of the surgical area, so that the surgeon can manipulate the surgical instruments as needed to complete the procedure. In the simplest sense, laparoscopic procedures are video-guided surgery.
Gynecological laparoscopic procedures can be used for diagnosis when you are experiencing pelvic pain or infertility. Gynecological laparoscopies can diagnose endometriosis, uterine fibroids, ovarian cysts or tumors, pelvic inflammatory disease, and reproductive cancers. Various treatments can also be administered using a laparoscopy, including: hysterectomy, endometrial tissue ablation, vault suspension for a prolapsed uterus, and the removal of ovarian cysts, fibroids, or the ovaries.
Robotic Procedures
These procedures use a tool known as the da Vinci Surgical System. Like laparoscopic procedures, robotic procedures are video-guided and require multiple tiny incisions in the abdomen for a camera and surgical instruments. However the main difference between laparoscopic and robotic surgery is that the surgeon performs the surgery by controlling the surgical instruments and camera through a console located next to the patient.
Robotic procedures can be used to diagnose and treat the same conditions as laparoscopic procedures, however the difference is that these procedures are performed with the robotic surgical system. During your surgery, your surgeon will be able to view a highly detailed, magnified image of your anatomy and control tiny surgical instruments to complete the procedure. These instruments are designed to move like a human hand, but with a greater range of motion. This makes them ideal for precisely completing complex and delicate procedures.
As you can see, each of these minimally invasive gynecological surgical procedures has its own unique approach for diagnosing and treating specific gynecologic conditions. Ultimately, the type of minimally invasive surgical procedure your gynecologist will recommend depends on a number of factors. For this reason, it is recommended to discuss your options in greater detail with your gynecological surgeon before committing to surgery.
As many as 25-45% of women experience urinary incontinence at least once a year. While older women are more likely to experience urinary incontinence, young and middle-aged women are also affected by this problem. Yet, many of these women believe that this is a normal part of aging or a consequence of giving birth. Because of this, many women don’t seek treatment for their symptoms since they don’t realize what is normal and what is not. Therefore, it is important to evaluate what is normal and what is not normal in order to determine if you could benefit from treatment.
What is normal?
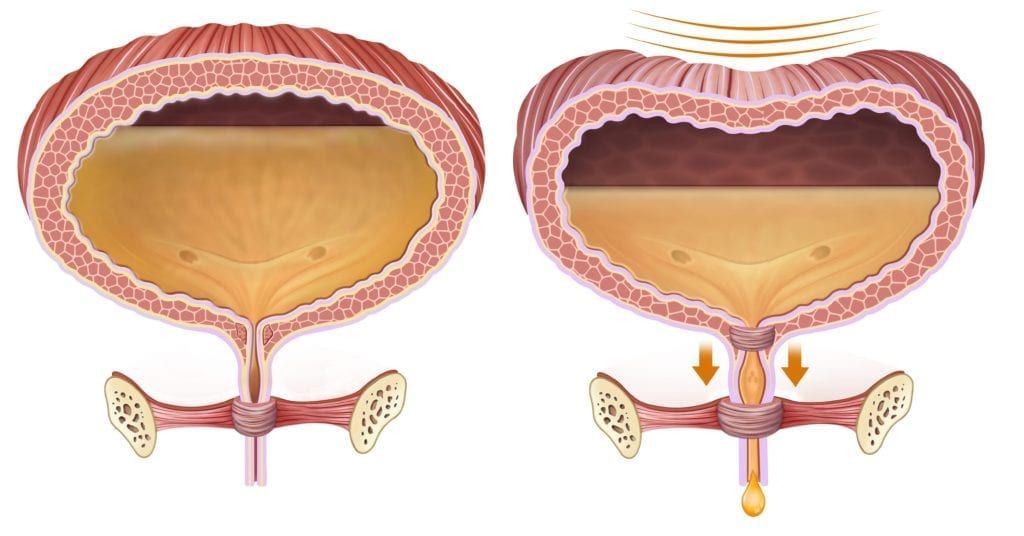
On average your bladder can hold around two cups of urine, which means that you will need to empty your bladder about 5-7 times during a 24 hour period. In older women, it is normal to urinate more frequently as bladder capacity decreases. This usually means that older women urinate about 8 times during the day and may wake once during the night to urinate.
As the bladder begins to stretch and fill with liquid, it is normal to experience the urge to urinate. However, urges are felt before the bladder is completely full and should be able to be controlled. Once urination begins, it is normal for urine to flow steadily without exertion or discomfort until the bladder has been emptied.
What is not normal?
Now that we have taken a closer look at what is normal for your bladder, let’s look at some abnormalities:
Frequent feelings of urgency followed by an inability to get to a bathroom in time (usually a few seconds or a few minutes warning)
Inability to urinate despite feeling the urge to urinate
Weak stream of urine or a stream that starts and stops
Feeling like you cannot empty your bladder completely
Experiencing a constant dribble of urine
What to do if you are experiencing symptoms:
In looking at what is normal and what is not normal for your bladder, you may have realized that you have been experiencing symptoms of urinary incontinence. Luckily, there are a variety of treatments available to manage your symptoms. The first step is to schedule an appointment with a urogynecologist to discuss your symptoms and receive a personalized treatment plan.
During your appointment, your urogynecologist will ask you to provide information about your medical history (including childbirths, procedures, surgeries, illnesses, or injuries), current health problems and medications, and whether you’ve ever had problems with your urinary system before. They will use this information to determine your individual treatment plan.
Although treatment plans can vary among the individual, some general guidelines may include:
Avoid drinking large amounts of liquids at once and instead drink small amounts somewhat frequently
Drink at least 6 cups of fluid daily
Limit or avoid caffeine, alcohol, carbonated drinks, and acidic foods/beverages
Practice exercising your pelvic floor muscles (Kegels)
In addition to these guidelines, your urogynecologist may also recommend other forms of treatment such as bladder training, electrical stimulation, estrogen creams, implants, medications to reduce feelings of urgency, or surgery. However, surgery is generally performed as a last resort option after a variety of conservative methods have failed.
While women primarily associate gynecological visits with their reproductive health, it is important to remember that gynecologists are also specialists in women’s health. This means that they are aware of certain medical conditions that may affect women differently or more frequently than men. For this reason, it is important to tell your gynecologist about symptoms you’ve been experiencing, even if you don’t think they are related to your reproductive health.
In fact, some symptoms you should never ignore are gastrointestinal (GI) symptoms, especially if these symptoms last longer than a few weeks, interrupt your sleep, or affect your daily routine. While some GI symptoms may be related to your reproductive health and can be treated by a gynecologist, others may require a referral to the appropriate specialist. Here are five GI symptoms that you should never ignore:
Abdominal Pain
When women experience abdominal pain, most of the time they just attribute it to being stomach pain. However, there are a number of other structures in the abdomen that can be the cause of abdominal pain. In fact, there are a number of other conditions that can cause severe abdominal pain, including: uterine fibroids, endometriosis, and cystitis. Therefore, it is important to tell your gynecologist if you’ve been experiencing abdominal pain, where the pain is coming from, and how long it has been going on.
Changes in Bowel Habits
Changes in how frequently you go, as well as changes in the consistency of your stools are also things you should mention to your doctor. Diarrhea, constipation, and painful bowel movements are also common symptoms of endometriosis. Unfortunately, many gastroenterologists tend to miss this diagnosis since they only look at the digestive tract. As a result, many women are incorrectly diagnosed with IBS.
Bloating
Bloating occurs when the GI tract fills with air and makes your abdomen feel full and tight. For many women, bloating is a common symptom of PMS since it tends to occur as a result of hormone fluctuations. For this reason, many women are not concerned about bloating. On its own, bloating usually isn’t serious. However, when accompanied by other GI symptoms, bloating could indicate a problem. In fact, bloating is one of the most common symptoms of endometriosis.
Frequent Heartburn
Despite the fact that there are a variety of over the counter ways to relieve heartburn, if you are experiencing heartburn regularly, you should mention this to your doctor. In some cases, heartburn can be a sign of pregnancy, since higher levels of progesterone relax the lower esophageal sphincter and allow stomach acid to escape into the esophagus.
Blood in the Stool
Seeing blood in your stool can be scary and it is definitely something you will want to mention to your doctor. There are a variety of reasons why you may have blood in your stool, ranging from hemorrhoids to cancer. Blood in the stool is also a common symptom associated with inflammatory bowel disease (IBD). In cases where endometriosis lesions have affected the bowel, this can also cause blood in the stool, as well as painful bowel movements.
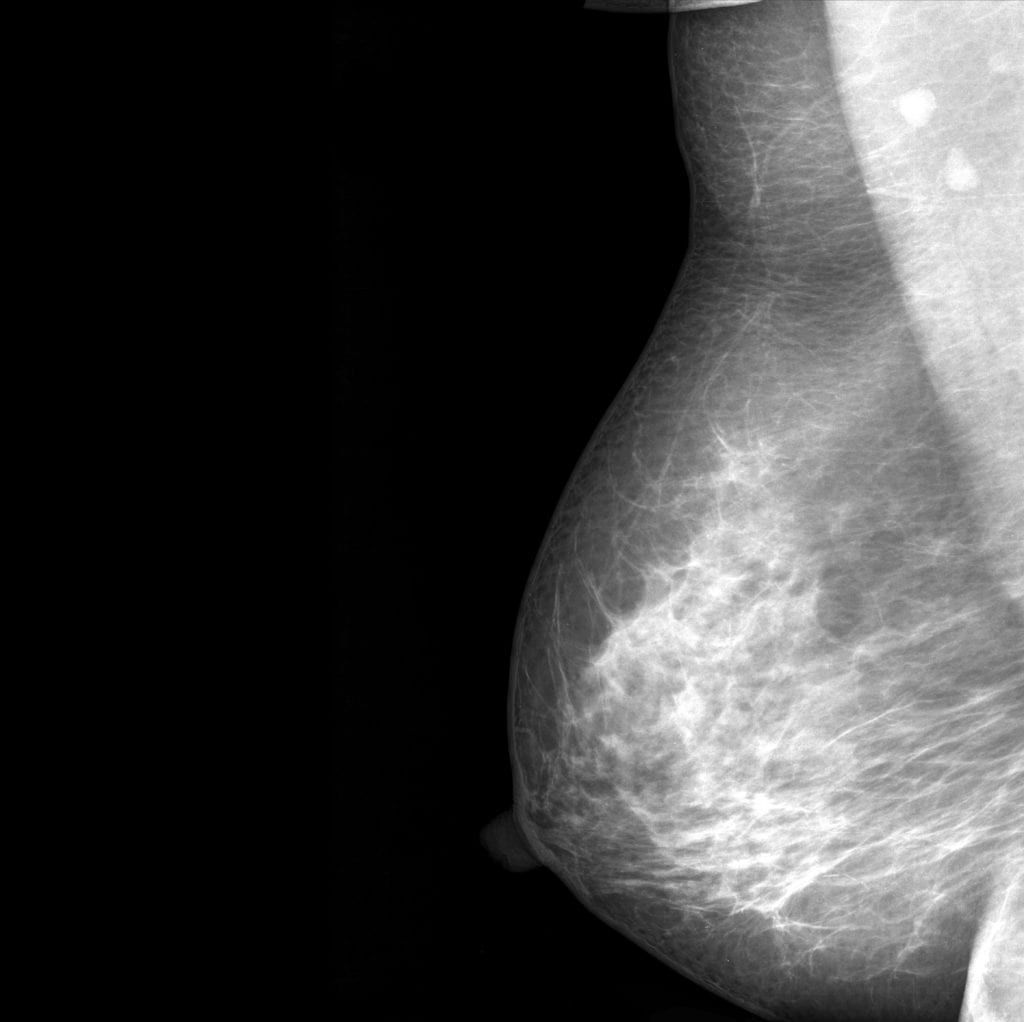
We all know that breasts come in a variety of shapes and sizes, but did you know that breasts can also vary in density? When it comes to breasts, density is not determined by size or firmness, rather it is determined by the ratio of fibroglandular tissue(lobules, ducts, and connective tissue) and fat in the breasts. Therefore, women whose breasts contain more than 50% fibroglandular tissue are said to be dense.
Because breast density is not determined based on size or firmness, it can only be determined during a mammogram. On a mammogram, dense breast tissue will simply look like a solid white area that can be difficult to see through. Radiologists who perform mammograms will use something known as theBreast Imaging Reporting and Data System (BI-RADS) in order to classify breast density. This system breaks down breast density into four categories, including:
A- Almost Entirely Fatty
Breasts that are categorized as type A are mainly composed of fatty tissue. Generally speaking, this means that they contain less than 25% of fibroglandular tissue. Only around 10% of women have type A breasts.
B- Scattered Areas of Fibroglandular Density
Breasts categorized as type B are also mostly composed of fat, however they also contain scattered areas of fibroglandular tissue that adds to the density of their breasts. Generally speaking, this means that their breasts contain about 25-50% fibroglandular tissue. About 40% of women have type B breasts.
C- Heterogeneously Dense
Breasts categorized as type C are composed primarily of fibroglandular tissue. In fact, they generally contain about 51-75% fibroglandular tissue. About 40% of women have type C breasts.
D- Extremely Dense
Breasts categorized as type D are almost entirely composed of fibroglandular tissue. In fact, they are composed of 75% or more fibroglandular tissue. Only about 10% of women have type D breasts.
As you can see, the majority of women tend to fall in the middle of the scale, meaning that most women have breasts composed of dense tissues. While scientists are not exactly sure why this happens, there are a few theories that can explain why some women have more dense breasts than others. One of the first theories is that age causes breast density to break down, especially after menopause. Along with age, it is also believed that hormones and body weight play a role in breast density as well. In fact, women taking hormone replacement therapy have been found to have an increase in breast density. Finally, women with lower body weights are more likely to have more dense breasts since they have a lower amount of fat overall.
It is important to note that having dense breasts may put you at an increased risk of developing breast cancer, and the denser your breasts, the higher this risk. In fact, dense breasts are a risk factor that is not well known by most women. In some cases, dense breasts can also be mistaken for a mass or a tumor, especially since all of these things cause a white shape on the mammogram. Unfortunately, mammograms also tend to be less accurate in women with dense breasts and 1 in screening mammograms will miss a breast cancer diagnosis.
Because of this, your doctor may perform a mammogram, as well as additional supplemental imaging to make sure your breasts are healthy. Other supplemental imaging techniques include an ultrasound, MRI, contrast enhanced mammography (CEM), and molecular breast imaging (MBI). It may also be helpful to request a 3D mammogram, since they can obtain a variety of clearer images from multiple angles. In fact, 3D mammograms are quickly becoming more popular.
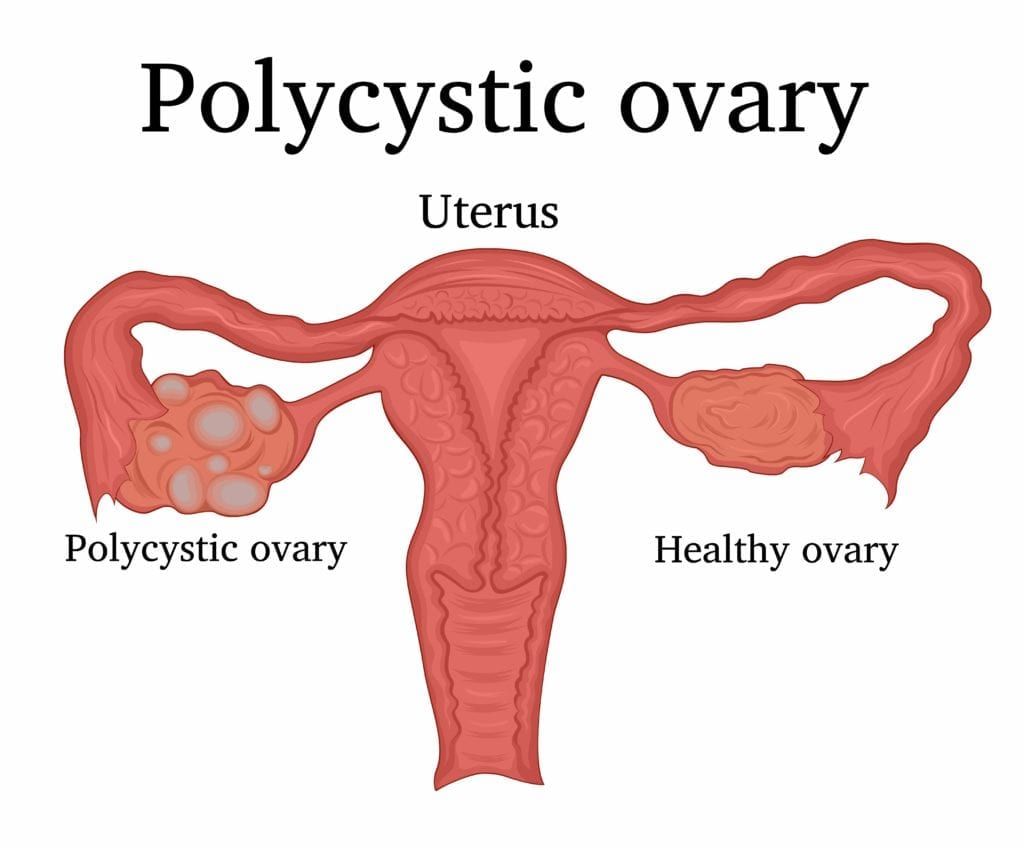
Did you know that one of the main treatments for polycystic ovary syndrome is dietary changes? This is because research has shown there is a strong link between diet and symptoms associated with PCOS. Specifically, certain foods can make symptoms worse, while others can help to alleviate symptoms. To understand why this is, we first need to take a closer look at PCOS.
Polycystic ovary syndrome is a condition that affects women’s hormone levels causing cysts in the ovaries, high levels of male hormones (androgens), and irregular or skipped periods. Since PCOS affects the ovaries and ovulation, it can also make it harder to get pregnant. The most common symptoms of PCOS include: irregular periods followed by periods of heavy bleeding, hair growth on the body and face, acne, weight gain, and thinning of the hair on the scalp.
These symptoms can be attributed to the increase in male hormones associated with PCOS. Although it is not exactly clear what causes an increase in the production of male hormones, one common link to excess androgen production is insulin resistance. In fact, close to 70% of women with PCOS are insulin resistant.
Insulin is a hormone produced by the pancreas and used by the body to convert sugar into energy. However, when one is insulin resistant, the body is unable to effectively convert sugar, meaning that it remains in the blood, causing high blood sugar. When the body senses high blood sugar, it produces more insulin as a way of trying to regain balance. The high amount of insulin then causes the ovaries to produce more androgen, which can exacerbate the symptoms of PCOS.
In addition to causing the ovaries to produce more androgen, high insulin levels can also cause metabolic syndrome, which is characterized by elevated cholesterol, blood sugar, and blood pressure. Oftentimes, metabolic syndrome can be a precursor to other medical conditions such as type II diabetes, stroke, and heart disease. This risk is further increased by obesity, which can be another potential complication of weight gain associated with PCOS.
Since PCOS and insulin resistance are so closely related, treatment generally consists of dietary changes that are beneficial for both conditions. At a glance, this means avoiding or minimizing refined carbohydrates such as starches and sugars. Additionally, it also means adding specific foods to your diet such as:
High-Fiber Foods
Dietary fiber is beneficial for managing insulin resistance and PCOS symptoms because it slows down digestion. Slowing digestion helps to reduce the effects of sugar on the blood. Examples of high-fiber foods to add to your diet include:
Almonds
Arugula
Beans and lentils
Berries
Broccoli
Brussels sprouts
Cauliflower
Green and red peppers
Pumpkin
Red leaf lettuce
Winter squash
Lean Proteins
Protein should make up another important part of your diet, however some protein sources are healthier than others. It is recommended to consume lean proteins that are lower in calories and fat than other proteins. These include:
Fish (Salmon & Sardines)
Skinless Chicken & Turkey
Tofu
Anti Inflammatory Foods
Our body experiences inflammation from time to time, as it is an important part of defending itself against infections. However, chronic inflammation can cause a variety of health problems. By eating antiinflammatory foods, you can help reduce inflammation and improve your overall health. These foods include:
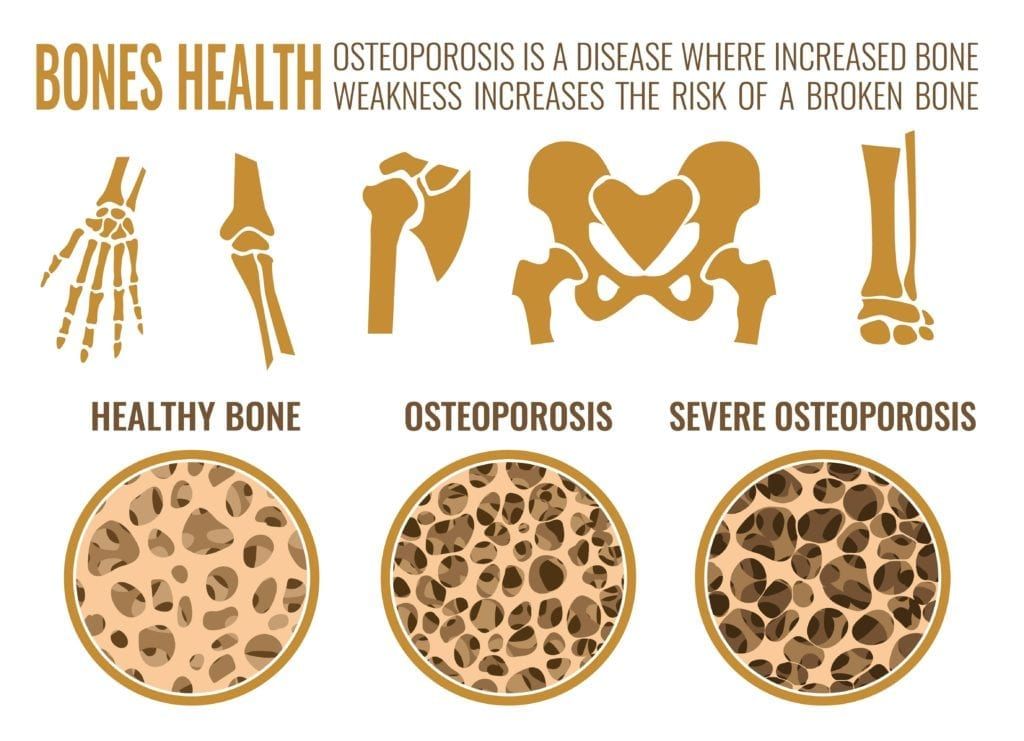
According to the National Osteoporosis Foundation, a woman’s risk of breaking a hip due to osteoporosis is equal to her risk of developing breast, ovarian, and uterine cancer combined. In fact, as many as 1 in 2 women will break a bone due to osteoporosis. Although many people think brittle bones are a natural part of aging, osteoporosis is actually a disease characterized by losing too much bone, making too little bone, or a combination of both.
Women are at a higher risk than men of developing osteoporosis due to their natural body structure. Generally speaking, women’s bones tend to be thinner than men’s bones, which means they have less bone to lose. Additionally women usually live longer than men, which is another reason why they tend to develop osteoporosis at a higher rate.
In addition to gender, there are also other risk factors for osteoporosis such as:
Age: bone density peaks at the age of 30, then starts to decrease. Women over the age of 50 are more likely to develop osteoporosis.
Family history of osteoporosis: women whose parents or grandparents had the disease are more likely to develop osteoporosis themselves.
Low body weight: women that are small-boned and thin have an increased risk of developing osteoporosis since they have less bone to lose.
Past broken bones: bones that have fractured before may be weaker and more susceptible to developing osteoporosis.
Ethnicity: Caucasian and Asian women are more likely to develop osteoporosis.
Taking certain medications: taking steroids for an extended period of time can increase the risk of osteoporosis
Unfortunately, the aforementioned risk factors cannot be controlled, with the exception of possibly changing medications. Therefore, it is important to focus on the things that you can control to reduce the risk of developing osteoporosis. Here are some ways to minimize your risk:
Get enough calcium and vitamin D: Calcium is an essential mineral for strong bones, while vitamin D is essential for calcium to be absorbed by the body. Unfortunately, many women are vitamin D deficient, meaning that they don’t get enough dietary vitamin D. this can minimize the amount of calcium absorbed by the body, which can increase the risk of osteoporosis.
Eat plenty of fruits and vegetables: Fruits and vegetables contain a number of important nutrients that support your overall health and decrease your risk of osteoporosis. At a glance, fruits and vegetables that contain vitamin D, vitamin C, vitamin K, potassium, magnesium, and omega 3s are especially important.
Be active: people who live a sedentary lifestyle are more likely to develop osteoporosis, so it is important that you get enough exercise. Even just walking for 30 minutes a day is enough to decrease your risk.
Quit smoking: Smoking has a number of health risks and being bad for your bones is just one of them.
Minimize alcohol intake: Drinking occasionally isn’t normally a problem, however excessive alcohol intake thins your bones and increases your risk of osteoporosis.
If you are reading this article, then you are probably aware of the fact that certain types of human papillomavirus (HPV) can cause cancer. But have you ever wondered why only certain types of HPV cause cancer? Or about how, exactly, these types of HPV go from being a virus to being cancerous?
In order to understand how HPV can cause cancer, we first need to take a look at the different types of HPV. There are two types of the virus: oncogenic and non-oncogenic. The oncogenic type is associated with the possibility of causing cancer, while the non-oncogenic has only been found to cause genital warts. Both oncogenic and non-oncogenic types of HPV often go unnoticed by the individuals they have infected since there may be no symptoms.
Since the virus can be asymptomatic, it tends to spread quickly from one individual to another. HPV is extremely common, to the point where the National Cancer Foundation estimates nearly all sexually active people are infected among becoming sexually active. The National Cancer Foundation also notes that about half of these infections are oncogenic.
However, being infected with the oncogenic type of HPV does not guarantee you will get cancer. In fact, the Centers for Disease Control and Prevention estimates that only 10% of women with HPV will develop the type of infection associated with cancer. This is because the majority of HPV infections are eliminated naturally by the body’s immune system within two years.
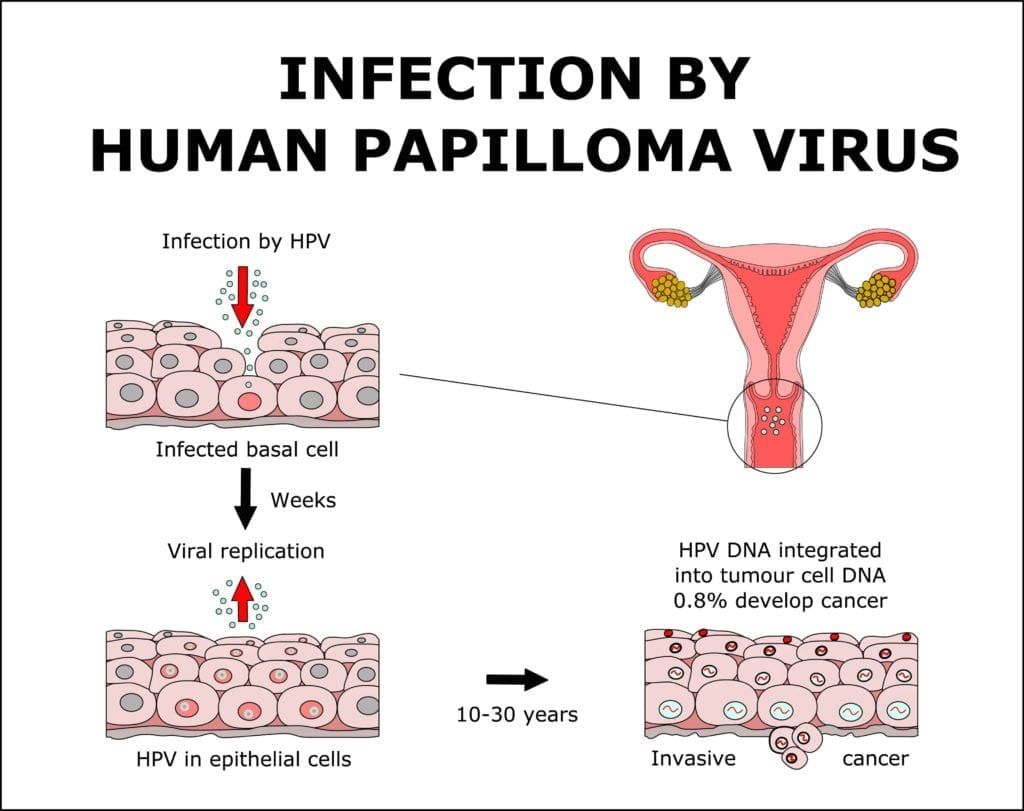
Still, there are some cases where the body’s immune system is unable to eliminate the HPV infection. When this HPV infection is oncogenic, it can eventually turn normal cells into abnormal cells, and then eventually into cancerous cells. HPV affects squamous cells found in the inner lining of the cervix, oropharynx (back of the throat, soft palate, base of the tongue, and tonsils), anus, rectum, vagina, and vulva. Therefore, most HPV-related cancers are known as squamous cell carcinoma. In cases where the gland cells of the cervix are affected, then it can be called adenocarcinoma.
Oncogenic HPV infections have the possibility of turning into:
Cervical cancer (almost 100% caused by HPV)
Oropharyngeal cancers (70% caused by HPV)
Anal cancer (90% caused by HPV)
Vaginal cancer (75% caused by HPV)
Vulvar cancer (70% caused by HPV)
To prevent HPV from turning into cancer, gynecologists perform screenings tests for cell changes. Currently, however, cervical cancer is the only type of HPV-caused cancer that has an FDA approved screening process. To screen for cervical cancer, your gynecologist will perform a pap smear where a sample of cervical cells is obtained by swabbing the cervix. This sample will then be sent to a laboratory, where it will be evaluated for the presence of high-risk HPV, as well as cervical cell changes.
In cases where cervical cell changes are observed, your gynecologist will be able to devise a treatment plan. Precancerous cells are easier to treat than cancerous cells, and early treatment may prevent cervical cancer from even happening. In most cases, additional testing will need to be completed to determine a specific diagnosis and the best treatment plan.
Many women see their primary care doctor for annual physicals and some may even elect to have their primary care doctor take care of their pap smears and pelvic exams. Since there is a definite overlap in some of the services provided by a primary care physician and a gynecologist, it can be tough to know when you should be seeing a gynecologist instead of your primary care physician.
In cases where you have no gynecological concerns or complaints, then choosing between your primary care physician and your gynecologist is simply a matter of comfort and convenience. For some, it is easier to only visit a single doctor, while others may want to have a specific doctor dealing with their gynecological health.
However, there may be some cases where seeing a gynecologist instead of your primary care physician is recommended. This is simply because a gynecologist specializes in women’s health, while primary care physicians have a broader focus. Some reasons to see a gynecologist over a primary care physician include:
Abnormal Pap Smears
Having a pap smear come back as abnormal doesn’t automatically mean you have cervical cancer. In fact, there are a variety of things that can cause an abnormal pap smear result. Still, your primary care physician may recommend visiting your local gynecologist to determine why the results were abnormal and possibly have another smear. Even if your primary care doctor does not refer you, it is recommended to see a gynecologist regarding abnormal pap smears.
Specialized Care
As mentioned before, primary care physicians have a broad scope of focus, while gynecologists focus exclusively on women’s health. This means that gynecologists may have information that your primary physician doesn’t. For example, while your primary physician can diagnose and monitor conditions like hypertension, diabetes, and thyroid disorders, a gynecologist can educate you about how these conditions affect your reproductive system and sex life.
You are having problems with infertility
If you have been trying to get pregnant for awhile and have not been successful, then it may be helpful to schedule an appointment with your gynecologist instead of your primary care doctor. This is because gynecologists have extended knowledge about the various ins and outs of the female reproductive system. They are also able to provide infertility treatments and help you to identify what is causing your infertility.
You Have Gynecological Complaints
If you are having problems related to any part of your reproductive system or related to your periods, then it may be time to see a gynecologist. While your primary care physician may be able to give you a general idea of what is going on, only a gynecologist can make sure you get an accurate diagnosis and the best treatment for the condition.
For a second opinion
If you feel like there is something “not quite right” about your reproductive system, then it is recommended to see a gynecologist even if your primary care physician says everything is fine. In getting a second opinion, your gynecologist may be able to detect something your primary care physician couldn’t.
We all have moments where we’re just “not in the mood”. But if you find yourself never being in the mood, it could be an indication that you are affected by hypoactive sexual desire disorder (HSDD), also known as female sexual interest/arousal disorder. HSDD is a type of sexual dysfunction classified by a little to no interest in sexual activity, lack of pleasure from genital stimulation or sex, little to no sexual thoughts or fantasies, or disinterest in initiating sex.
HSDD can have physical or emotional causes, as well as a combination of both. Therefore, treatment for HSDD works by identifying and addressing these causes. For emotional causes, such as anxiety, depression, self-esteem issues, trust issues, or history of sexual abuse, working with a mental health professional is generally recommended. However, if HSDD has a physical cause, then the best treatment is to diagnose and treat the underlying medical condition. Here are some common medical conditions that can be hindering your sexual desire and causing HSDD:
Diabetes
Type-2 diabetes can cause hormone changes, as well as reduced blood flow to the genitals. As a result, vaginal dryness can occur and make sex painful. It has also been found that women with diabetes have an increased risk of developing vaginal inflammation, vaginal infections, and urinary tract infections (UTIs).
Heart Disease
Poor circulation can disrupt blood flow to the genitals, resulting in a lack of lubrication and arousal. Unfortunately some of the medications used to treat heart disease can also dampen desire, as well as make it more difficult to achieve orgasm. In some cases, different medications can be used to alleviate sexual dysfunction.
High Blood Pressure
While the link between high blood pressure and sexual problems in women is not exactly clear, there is some evidence to suggest that high blood pressure can cause vaginal dryness, a decrease in sexual arousal and difficulty achieving orgasm.
Hormone Changes
If you just had a baby and are currently breast-feeding, your prolactin levels are higher to promote breast milk production. However, high prolactin levels causes the hormones responsible for sex drive to drop. Post-menopausal women and women transiting into menopause also undergo a decrease in the hormones responsible for sex drive. Often times, the other medical conditions in this list may also cause your hormones to fluctuate and affect your libido.
Neurological Conditions
Sexual dysfunction can occur as a symptom of a neurological disorder, as well as an effect of one and only a consultation with a neurologist can determine which it is. Most commonly, sexual dysfunction associated with neurological conditions occurs as a decrease in sexual desire, vaginal dryness, or inability to experience sexual pleasure. In some cases, an unusual increase is sex drive can also indicate a neurological condition.
Thyroid Problems
Thyroid disease can lower vaginal lubrication, which can make sex less pleasurable and even painful in some cases. Thyroid disease also decreases testosterone levels, which lowers your sex drive. While many people think testosterone is a male hormone, women produce this hormone as well. In both males and females, testosterone plays an important role in regulating sex drive. Finally, both hyperthyroidism and hypothyroidism can cause depression and fatigue, which have both been found to negatively affect sex drive.